Key Difference Between Acute and Chronic GVHD
Acute and Chronic GVHD involves the immune system attacking the recipient’s tissues after transplantation.
Graft-versus-host disease (GVHD) often arises following transplant procedures. Acute cases usually emerge within 100 days due to donor immune cells attacking host tissues; it manifests with skin rashes, digestive distress, and liver problems as symptoms. Chronic GVHD typically appears later, and shares many features with autoimmune conditions.
It affects the skin, mucous membranes, organs, and multiple systems beyond 100 days post-transplant and typically manifests gradually before eventually manifesting as symptoms resembling an autoimmune condition and often manifesting with lung, joint, and eye involvement.
Diagnostic criteria include clinical evaluation, biopsies, and various specialized tests. Treatment typically entails immune suppression while chronic GVHD requires long-term management; advances in research aim to advance diagnosis, therapy, and patient outcomes of acute and chronic GVHD alike.
What is Acute GVHD?
Graft-versus-host disease (GVHD), is one of the major risks involved with transplanting blood or bone marrow stem cells and occurs when donor immune cells identify recipient tissues as foreign and launch an attack upon them. Adverse Graft-versus-Host Disease, more commonly referred to as acute GVHD, typically strikes within 100 days after transplantation and affects the skin, digestive system and liver systems.
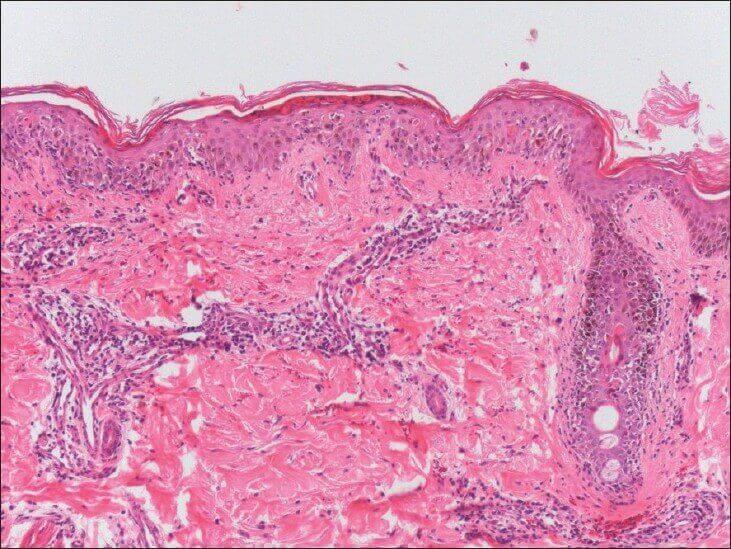
Diagnostic of acute GVHD involves clinical assessment, supplemented by skin and gut biopsies to reveal characteristic histopathological features. Corticosteroids tend to be used as the first-line treatment option. Response to treatment varies, with additional therapeutic approaches often necessary in refractory cases. Researchers continually work on refining diagnostic methods, optimizing treatment strategies and better comprehending immune-based processes.
Yet acute GVHD continues to pose serious obstacles in transplant medicine despite improvements that demonstrate its importance – emphasizing why continued research efforts must continue to ensure better patient outcomes.
What is Chronic GVHD?
Chronic Graft-versus-Host Disease (GVHD) is a medical condition that may develop following stem cell or bone marrow transplant when donor immune cells recognize the recipient body as foreign and create an immune response against them. Although acute GVHD typically develops shortly after transplantation, chronic forms often arise months to years later and resemble an autoimmune disease by attacking various organs and tissues within it.
This includes skin, mucous membranes, liver lungs joints as well as other systems within. Symptoms range widely including skin rashes dry eyes mouth sores joint pain as well as others. Diagnostic of chronic GVHD often involves clinical evaluation and requires biopsies of affected tissues for confirmation. Treatment generally entails suppressing immune responses in order to relieve symptoms and stop further damage.
Often using corticosteroids and immune-modulating drugs as immunosuppressants; finding the ideal balance between managing chronic GVHD symptoms and infection prevention can be tricky Regular follow-up by physicians is needed so treatments may be adjusted appropriately as needed ongoing research aims to improve understanding, diagnosis, and management in order to enhance the quality of life for transplant recipients.
Acute GVHD: Causes, Symptoms, and Characteristics
Graft-versus-Host Disease (GVHD) in Acute Form: Causes, Symptoms and Characteristics:
Causes:
Graft-versus-host disease (GVHD), also known as Graft versus Host Syndrome, is an unpleasant complication after stem cell or bone marrow transplant surgery that develops when immune cells from the donor identify certain tissues of their recipient (host) as foreign and trigger an immune reaction against them; mismatch between donor and recipient tissue types often sets this off.
Symptoms:
Acute Graft-Versus-Host Disease (GVHD) affects primarily the skin, gastrointestinal tract, and liver of its recipients. Symptoms may range in intensity but typically consist of skin rashes, blistering diarrhea nausea vomiting abdominal pain or jaundice caused by their immune systems attacking tissues in their recipient.
Characteristics:
- Timing: Acute GVHD typically manifests within 100 days following transplant, due to rapid activation of donor immune cells.
- Severity: Symptoms may range in intensity from mild, with limited skin involvement, to severe organ involvement and life-threatening complications.
- Skin Involvement: Skin symptoms often present as rashes or blistering similar to conditions like dermatitis or erythema.
- Gastrointestinal Involvement: Gastrointestinal symptoms often include diarrhea, nausea, vomiting and abdominal pain from inflammation or damage in the digestive tract.
- Liver Complications: Jaundice can occur due to liver involvement. Elevated liver enzyme levels may also increase.
- Diagnosis: Diagnosis of acute GVHD requires clinical assessment of symptoms as well as skin and gut biopsies to confirm immune cell infiltration.
- Treatment: Immunosuppressive medicines such as corticosteroids are the cornerstone of treatment, acting to dampen immune response and alleviate symptoms.
- Response Variability: Individual responses can differ and, in certain instances, initial therapies may not work, necessitating additional strategies as an intervention option.
- Prophylactic Measures for Acquired GVHD: Strategies to prevent acute GVHD include donor/recipient matching, immune suppressants medications and careful observation.
- Research: Ongoing research seeks to increase our understanding of underlying mechanisms, refine treatment protocols and develop targeted therapies.
Chronic GVHD: Causes, Symptoms, and Characteristics
Chronic Graft-versus-Host Disease (GVHD): Causes, Symptoms and Characteristics :
Causes:
Chronic Graft-versus-Host Disease (GVHD) often develops post stem cell or bone marrow transplantation when immune cells from the donor continue to attack recipient tissues despite initial attempts at immune suppression by treatment protocols or independently due to ongoing immune dysregulation and tissue damage. It can either develop as an extension of acute GVHD or independently due to ongoing immune dysregulation and tissue destruction.
Symptoms:
Chronic GVHD affects multiple organs and systems, frequently mimicking an autoimmune disease. Common signs and symptoms may include persistent skin changes like rashes or tightness; dry eyes, and mouth leading to discomfort; joint pain, muscle weakness, breathing difficulties due to lung involvement; digestive disorders, liver dysfunction as well as potential liver dysfunction.
Characteristics of Chronic Graft-Versus-Host Disease (GVHD)
- Delayed Onset: As opposed to acute GVHD, chronic GVHD often develops months to years post-transplant during recovery or sometimes beyond this phase.
- Persistence of Chronic GVHD: Chronic GVHD is an ongoing condition that may impact the recipient’s quality of life for an extended period.
- Autoimmune Features: Chronic GVHD shares many similarities with autoimmune diseases in terms of its immune response: immune cells attacking its own tissues.
- Organ Involvement: Chronic GVHD may impact numerous organs including skin, mucous membranes, liver, lungs, digestive tract, and the musculoskeletal system.
- Varying Symptoms: Symptoms can range from mild to severe and vary with time, making diagnosis and management even more complicated.
- Overlapping with Acute GVHD: Chronic GVHD can develop from acute GVHD, and there may be symptoms that overlap, necessitating careful differentiation to accurately diagnose.
- Diagnosis: Clinical examination aided by biopsies is necessary for accurate diagnosis due to its wide-ranging and often-ambiguous presentation of symptoms.
- Treatment: Treatment involves immunosuppressive medication similar to acute GVHD to manage symptoms and limit further damage, phototherapy or targeted therapies may also be employed for specific symptoms.
- Long-Term Management of Chronic GVHD: Monitoring symptoms, tailoring treatments to individual cases and anticipating potential complications is required for effective chronic GVHD management and follow-up.
- Research and Advancements: Current research efforts aim to enhance our knowledge of chronic GVHD’s mechanisms while creating more efficient treatment approaches in order to enhance patient health outcomes and well-being.
Comparison between Acute and Chronic GVHD
Here’s a concise comparison chart highlighting the key differences between Acute and Chronic Graft-versus-Host Disease (GVHD):
| Aspect | Acute GVHD | Chronic GVHD |
|---|---|---|
| Onset | Within first 100 days post-transplant | Months to years after transplantation |
| Causes | Donor immune cells attack recipient tissues | Ongoing immune dysregulation |
| Primary Targets | Skin, GI tract, liver | Skin, mucous membranes, multiple organs |
| Symptom Timing | Rapid onset | Delayed onset |
| Symptom Severity | Can be life-threatening | Variable, can range from mild to severe |
| Characteristics | Immune response to foreign tissues | Resembles autoimmune diseases |
| Treatment | Immunosuppressive therapy, steroids | Immunosuppressive therapy, tailored meds |
| Response Variability | Varies among individuals | Varies among individuals |
| Long-Term Nature | Often resolves or becomes chronic | Chronic condition, may persist indefinitely |
| Diagnostic Approach | Clinical evaluation, biopsies | Clinical evaluation, biopsies |
| Overlap with Acute GVHD | May develop from acute GVHD | Can develop from acute GVHD, overlaps |
| Management Focus | Immune suppression, symptom control | Immune suppression, symptom management |
What are the Similarities Between Acute and Chronic GVHD?
Here is an outline of the differences between Acute and Chronic Graft-versus-Host Disease (GVHD).
- Immune Response: Both acute and chronic GVHD result from immune cells of a donor recognizing recipient tissues as foreign and mounting an attack against them, initiating an immune response.
- Post-Transplant Cause: Both conditions stem from stem cell or bone marrow transplantations, where donor cells interact with recipient’s bodies.
- Inflammation: Both acute and chronic GVHD involve an immune response which leads to inflammation. This results in damage being done to multiple organs and tissues by this immune response, ultimately contributing to damage being sustained from it.
- Diagnostic Challenges: Both forms of GVHD can be challenging to diagnose due to overlapped symptoms, the need for clinical evaluation and often biopsies in order to distinguish it from other conditions, or its overlapping symptoms that mask their signs and symptoms.
- Immunosuppression: One approach for treating acute and chronic GVHD involves using immunosuppressant medication to diminish immune reactions and manage symptoms.
- Variable Response to Therapy: Individual responses can differ widely when treating both acute and chronic GVHD; some cases being more responsive than others to therapy.
- Long-Term Management: Both conditions may need long-term monitoring to monitor symptoms, adjust treatment accordingly and address potential complications.
- Research Focus: Ongoing efforts aim to advance understanding of both acute and chronic GVHD, optimize treatment protocols, and develop therapies with targeted mechanisms of action for enhanced patient outcomes.
What are the treatments for Acute GVHD and Chronic GVHD
Acute GVHD: Treatment for Acute Graft-versus-Host Disease (GVHD) typically entails taking an interdisciplinary approach aimed at controlling immune activity and alleviating symptoms. Corticosteroids are the cornerstone therapy, effectively dampening down any immune activity. If necessary or unresponsive to corticosteroids, additional immunosuppressant medication like calcineurin inhibitors may be employed.
Additional supportive care including hydration, nutrition, and infection prevention services play a significant part too targeted therapies or novel interventions under research can often have positive outcomes as soon as they start being implemented quickly – making early detection essential in managing treatment outcomes successfully.
Chronic GVHD: Chronic Graft-versus-Host Disease (GVHD) must be managed comprehensively and individually; immunosuppressive therapies like corticosteroids and immune-modulating drugs aim to limit an autoimmune attack against various organs in its various manifestations.
Phototherapy may be useful in treating skin symptoms; treatment plans vary according to organ involvement and severity of symptoms, and regular follow-up is required in order to monitor symptoms that develop as well as potential complications that might arise over time.
Physical therapy, occupational therapy, and psychological support may all work to promote patients’ overall well-being. Research endeavors focus on understanding GVHD mechanisms and developing targeted treatments in order to offer improved quality of life for individuals living with the disorder.
Research and Advancements
Ongoing research and advancements aim to further our knowledge and treatment of both acute and chronic forms of GVHD. For Acute GVHD specifically, studies are delving more precisely into risk stratification to enable more tailored therapies and tailored treatment plans novel immunomodulatory agents are being researched alongside existing ones so as to counter resistance; furthermore, biomarker identification techniques provide early detection and intervention capabilities.
Research efforts are uncovering the immune mechanisms underlying chronic GVHD’s complex pathophysiology. Therapeutic strategies targeting specific immune pathways are being created in order to attenuate an autoimmune response while simultaneously decreasing generalized immunosuppression.
Cell therapies, like mesenchymal stromal cells, show promise as potential ways of managing Chronic GVHD symptoms effectively and on schedule. Research efforts also strive towards refining diagnostic criteria so as to enable more precise, timely diagnoses as well as proactive management measures.
Summary
Research in Genital Herpes Virus Deficit Disorder is producing innovative treatments for Acute and Chronic forms. Customized therapies, risk stratification tools and immunomodulatory agents are being investigated in Acute cases; while for Chronic forms.
Targeted therapies including immunopathogenic cell therapies address immune pathways and symptoms while diagnostic improvements aid early detection; collaborative efforts provide for improved outcomes and higher quality of life among affected individuals.